Anticholinergic drugs
Anticholinergic drugs are commonly used in respiratory medicine, especially in COPD and asthma. To understand how they work, we must first understand the cholinergic system
Fundamentals
Before we jump directly to Anticholinergics, let us first understand this term cholinergic, So that those who are completely unaware of everything (beginner) can understand.
What Is “Cholinergic”?
The term cholinergic refers to anything related to acetylcholine (ACh). Acetylcholine (ACh) is a neurotransmitter. A chemical messenger that carries signals between nerve cells and from nerves to muscles and glands.
A cholinergic system:
- Uses acetylcholine as a neurotransmitter
- Acts on cholinergic receptors (Nicotinic Receptors (Nn, Nm) And Muscarinic Receptors (M1-5))
- Is mainly part of the parasympathetic nervous system.
The Parasympathetic Nervous System (PNS) is a part of the autonomic nervous system (ANS) responsible for “Rest and Digest” functions. These are the functions of the nervous system when there is no emergency.
What Does the Cholinergic System Do?
As it is a main part of parasympathetic nervous system, So, its function is the same as that of the parasympathetic nervous system.
The parasympathetic (cholinergic) system is responsible for:
The Rest and Digest functions are
Effects in Different Organs:
| Organ | Effect of Acetylcholine |
|---|---|
| Heart | Lowers Heart rate |
| Lungs | Bronchoconstriction |
| Glands | Increases Secretions |
| GI tract | Increases Motility |
| Bladder | Contraction |
| Eye | Pupil constriction |
Easy Mnemonic For workings of Cholinergic System
“SLUDD”
- S – Salivation
- L – Lacrimation
- U – Urination
- D – Digestion
- D – Defecation
How Does It Work?
Acetylcholine acts on two types of receptors:
Muscarinic Receptors (M1–M5)
These are G-protein coupled receptors (GPCRs).They are categorized as M1, M2, M3, M4 & M5
| Receptor | Location | Action |
|---|---|---|
| M1 | CNS, stomach | Increases Gastric secretion |
| M2 | Heart | decreases Heart rate |
| M3 | Glands, smooth muscle | Increases Secretions, bronchoconstriction |
| M4, M5 | CNS | Modulatory role |
Nicotinic Receptors
These are the Ion channels, which are found in Neuromuscular junction and Autonomic ganglia
Now let’s move to main part of the topic
What Does “Anticholinergic” Mean?
Anticholinergic drugs are the drugs which block the action of acetylcholine.They block muscarinic receptors (especially M3) that’s why they are also known as Muscarinic Antagonists
Mechanism of Action of Anticholinergics

Normal pathway in the absence of Anticholinergics is as follows:
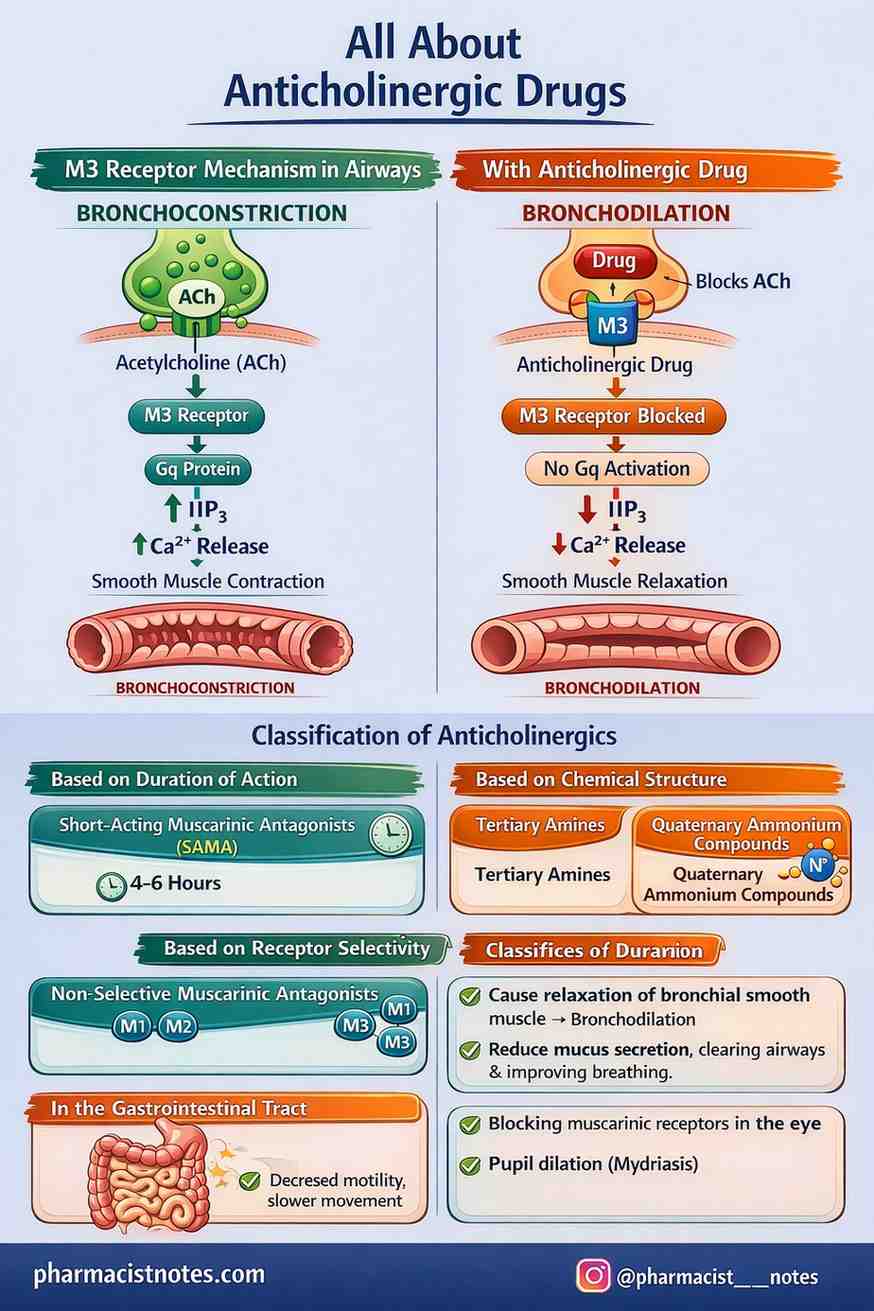
- acetylcholine (ACh) is released and binds to the M3 receptor present on smooth muscle cells in the bronchi.
- Once acetylcholine attaches to the M3 receptor, it activates a Gq protein inside the cell. This activation stimulates the production of IP₃ (inositol triphosphate).
- IP₃ then causes the release of calcium ions (Ca²⁺) from intracellular stores. As the calcium level inside the cell increases, the smooth muscle contracts.
- When this happens in the airways, the bronchial smooth muscles tighten, leading to bronchoconstriction (narrowing of the airways).
In simple terms, Acetylcholine → M3 receptor → Gq activation → IP₃ ↑ → Ca²⁺ ↑ → Smooth muscle contraction → Bronchoconstriction
With anticholinergic drug:
- When a drug binds to the M3 receptor, it prevents acetylcholine from attaching to that receptor.
- Because acetylcholine cannot bind, the Gq protein inside the cell is not activated. Without Gq activation, the formation of IP₃ (inositol triphosphate) decreases.
- As IP₃ levels fall, less calcium (Ca²⁺) is released inside the cell. Since intracellular calcium is responsible for smooth muscle contraction, its reduction leads to relaxation of the smooth muscle.
In simple terms, Drug binds to M3 receptor → Blocks acetylcholine binding → Prevents Gq activation → ↓ IP₃ formation → ↓ Intracellular Ca²⁺ → Smooth muscle relaxation → Bronchodilation
Classification of Anticholinergics
- Based on Duration of Action
- Short-Acting Muscarinic Antagonists (SAMA)
- Long-Acting Muscarinic Antagonists (LAMA)
- Based on Chemical Structure
- Tertiary Amines
- Quaternary Ammonium Compounds
- Based on Receptor Selectivity
- Non-Selective Muscarinic Antagonists
- Functionally M3-Selective (Kinetic Selectivity)

Now, It’s time to explain them one by one
1. Based on Duration of Action
a) Short-Acting Muscarinic Antagonists (SAMA)
These medicines work for a shorter duration, usually about 4 to 6 hours.
A common example is ipratropium.
They are mainly used for quick relief of symptoms, especially during sudden worsening of breathing problems, such as in COPD exacerbations. Because they act fast but don’t last very long, they are helpful when immediate symptom control is needed.
b) Long-Acting Muscarinic Antagonists (LAMA)
These drugs work for a much longer time — around 24 hours.
Examples include tiotropium, glycopyrronium, and umeclidinium.
They are mainly used for maintenance therapy, especially in patients with COPD. This means they are taken regularly every day to keep the airways open and prevent symptoms, rather than to treat sudden attacks.
In short,
- SAMA = Short-term relief
- LAMA = Long-term control
2. Based on Chemical Structure
a) Tertiary Amines
These drugs are lipid soluble, meaning they can easily pass through cell membranes. Because of this property, they are able to cross the blood-brain barrier (BBB) and enter the brain.
As a result, they are more likely to produce central nervous system (CNS) effects, such as confusion, sedation, or agitation (especially in elderly patients).
A common example is atropine.
b) Quaternary Ammonium Compounds
These drugs have poor lipid solubility, so they do not easily cross cell membranes. Because of this, they do not cross the blood-brain barrier.
Since they cannot enter the brain easily, they produce fewer CNS side effects.
Examples include ipratropium and tiotropium.
Most inhaled respiratory muscarinic antagonists belong to this group, which makes them safer in terms of central side effects.
3. Based on Receptor Selectivity
a) Non-Selective Muscarinic Antagonists
These drugs block all three main muscarinic receptors — M1, M2, and M3.
An example is ipratropium.
Since they do not differentiate much between receptor types, they block all of them more or less equally. Their effect is useful, but it is not specifically targeted toward one receptor subtype.
b) Functionally M3-Selective (Kinetic Selectivity)
An example of this is tiotropium.
Tiotropium is not absolutely selective in binding, but it shows what we call kinetic selectivity. This means it stays attached to certain receptors longer than others.
The important concept is:
- Tiotropium dissociates slowly from M3 receptors
- But it dissociates faster from M2 receptors
Because of this behavior:
It produces a long-lasting effect
It causes less interference with M2 auto-receptors, which are important for regulating acetylcholine release
So, even though it can bind to multiple receptors, its longer action on M3 makes it functionally more targeted and clinically more effective for long-term control.
Pharmacological Effects

Muscarinic antagonists produce different effects in different organs because they block acetylcholine at muscarinic receptors.
In the Lungs
These drugs cause relaxation of bronchial smooth muscle, which leads to bronchodilation.
They also reduce mucus secretion, helping to keep the airways clearer and improving breathing.
In the Heart
By blocking M2 receptors, they slightly reduce parasympathetic influence on the heart.
As a result, there may be a mild increase in heart rate.
In the Eye
Blocking muscarinic receptors in the eye can lead to pupil dilation (mydriasis).
In the Gastrointestinal Tract
They reduce parasympathetic activity in the gut, which leads to decreased motility and slower movement of food through the digestive system.
Clinical Uses
Muscarinic antagonists are widely used in different clinical conditions because they reduce parasympathetic activity in various organs.
COPD (Primary Use)
Anticholinergic drugs are considered first-line therapy in COPD.
The reason is that in COPD, vagal tone plays a major role in causing bronchoconstriction. By blocking muscarinic receptors, these drugs reduce vagal-mediated airway narrowing and help keep the airways open. That’s why they are especially effective and commonly prescribed in COPD patients.
For, what is COPD? how it happens? Pharmacotherapeutics of COPD click here
Asthma
In asthma, anticholinergics are usually not first-line, but they are used as add-on therapy, particularly in moderate to severe cases or during acute exacerbations.
They are often combined with beta-Agonists for better bronchodilation.
Other Uses
These drugs are also used in conditions outside the lungs:
- Atropine is used to treat bradycardia, as it increases heart rate by blocking M2 receptors in the heart.
- Glycopyrrolate is commonly used in anesthesia to reduce secretions and prevent reflex bradycardia.
- Oxybutynin is used for overactive bladder, as it relaxes the bladder muscle and reduces urgency and frequency.
Adverse Effects
Muscarinic antagonists block parasympathetic activity in the body. While this is helpful in treating certain conditions, it can also reduce normal parasympathetic functions, leading to side effects.
Common Adverse Effects
- Dry mouth – Because these drugs reduce salivary gland secretion.
- Constipation – Due to decreased gastrointestinal motility.
- Blurred vision – From pupil dilation and loss of accommodation.
- Urinary retention – Because bladder contraction is reduced.
- Tachycardia – Due to blockade of M2 receptors in the heart.
Why Do These Adverse Effects Occur?
All these side effects happen because muscarinic antagonists block acetylcholine at muscarinic receptors, reducing normal “rest and digest” functions of the parasympathetic system.
In simple words, when parasympathetic activity is suppressed, secretions decrease, smooth muscles relax, and certain normal body functions slow down — which leads to these predictable adverse effects.
Drug Interactions (Muscarinic Antagonists)
Muscarinic antagonists can interact with other medications mainly because they block acetylcholine and reduce parasympathetic activity. When combined with certain drugs, their effects may increase or oppose each other.
1. Other Anticholinergic Drugs
Examples:
- First-generation antihistamines
- Tricyclic antidepressants
- Antipsychotics
When taken together, anticholinergic side effects increase — such as dry mouth, constipation, urinary retention, blurred vision, and confusion (especially in elderly patients).
Why?
Because both drugs reduce parasympathetic activity, leading to an additive effect.
2. Cholinergic Drugs
Examples:
- Bethanechol
- Neostigmine
These drugs increase acetylcholine activity, which is the opposite of what muscarinic antagonists do.
Why does interaction occur?
They counteract each other’s effects, so the therapeutic response of one or both drugs may decrease.
3. Beta-2 Agonists (e.g., Salbutamol)
When used with Beta-2 Agonists (common in COPD and asthma), they can produce enhanced bronchodilation.
Why?
Because they work through different mechanisms — one blocks muscarinic receptors, and the other stimulates beta-2 receptors — leading to a combined airway-relaxing effect.
4. Drugs That Increase Heart Rate
Examples:
- Sympathomimetics
There may be an increased risk of tachycardia.
Why?
Muscarinic antagonists reduce parasympathetic control of the heart, and sympathomimetics stimulate the heart — together, they can significantly raise heart rate.


2 thoughts on “Anticholinergic drugs (Muscarinic Antagonists): Mechanism, Classification and Clinical Uses”