Bronchodilators Mechanism and Classification
What are Bronchi?
Bronchi are the main air tubes inside the lungs.
Nose → Trachea → Bronchi → Bronchioles → Alveoli
Bronchi carry air from trachea into both lungs.
They divide into smaller branches called bronchioles.

How do Bronchi get damaged?
Bronchi get damaged due to long-term irritation.
Main causes:
- Smoking
- Air pollution
- Dust exposure
- Infection
- Allergy
These irritants damage the airway lining (epithelium).
When damage happens:
- Immune system activates
- Inflammation occurs
- Airway wall becomes thick
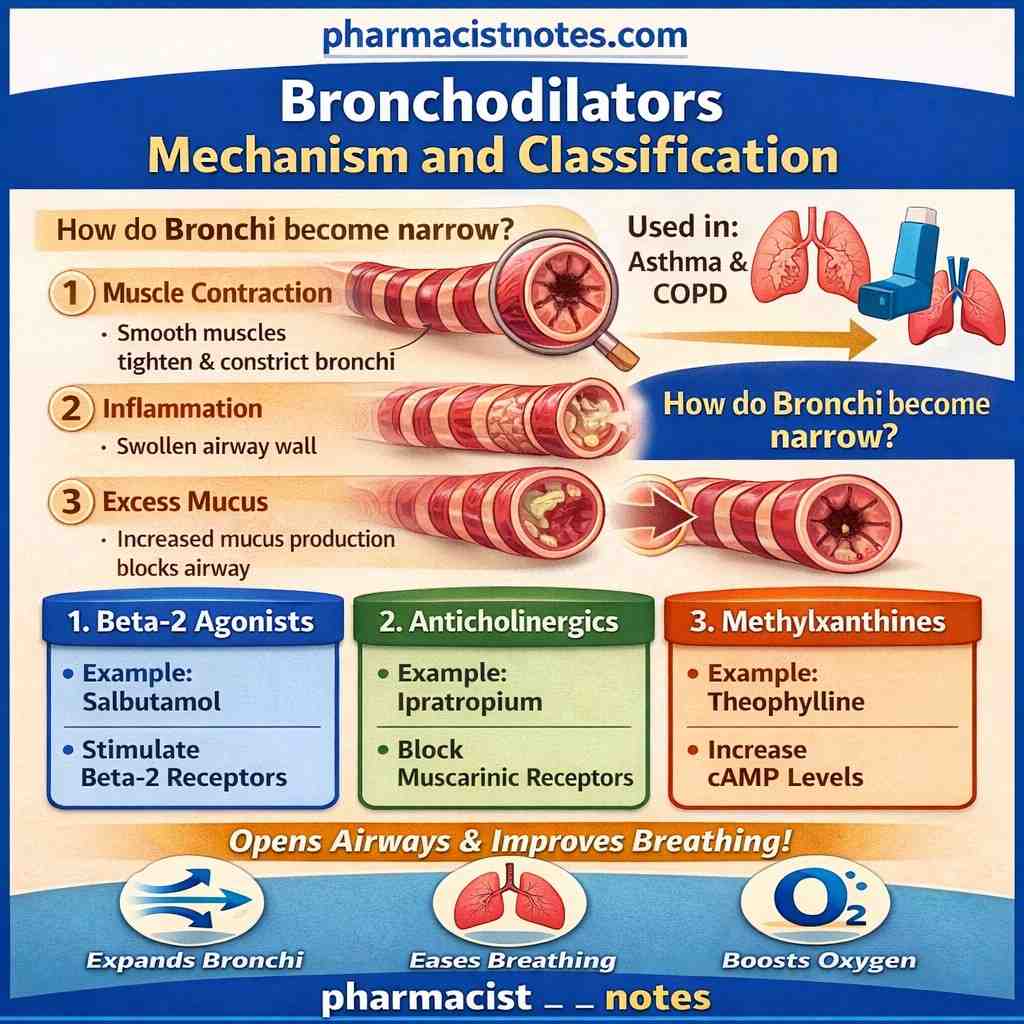
How do Bronchi become narrow?
Bronchi narrow for 3 main reasons:
1. Muscle contraction
Bronchial wall has smooth muscles.
When they contract → airway becomes narrow.
2. Swelling (Inflammation)
Airway lining becomes swollen due to inflammation.
3. Excess mucus
More mucus is produced → blocks airflow.
Result of Narrowing
When bronchi become narrow:
- Air cannot flow properly
- Patient feels breathlessness
- Wheezing sound occurs
- Oxygen supply decreases
What are Bronchodilators?Severe cases may cause hypoxia – a dangerous condition where body tissues are deprived of adequate oxygen, causing symptoms like confusion, rapid heart rate, shortness of breath, and blue-tinted skin (cyanosis).
What are Bronchodilators?
Bronchodilators are drugs that relax bronchial smooth muscles and widen the airways.
Broncho = BronchusDilator = To open
So:
Bronchodilators open narrowed airways and make breathing easier.
They are mainly used in:
- COPD
- Asthma
- Bronchospasm
High-Level Classification of Bronchodilators
Bronchodilators are divided into three main classes:
- Beta-2 Agonists
- Anticholinergics
- Methylxanthines

Beta-2 Agonists
Beta-2 receptors are present on the smooth muscles of the bronchi. When these receptors are stimulated, the airway muscles relax and the bronchi widen.
Beta-2 Agonists are further classified into following categories
- Based on Duration of Action
- Short-Acting β₂-Agonists (SABA)
- Long-Acting β₂-Agonists (LABA)
- Ultra-Long-Acting β₂-Agonists
- Based on Chemical Structure
- Catecholamines
- Non-Catecholamines
- Based on Selectivity
- Selective β₂ Agonists
- Non-Selective β Agonists
- Based on Lipophilicity
- Hydrophilic Drugs
- Lipophilic Drugs
- Intrinsic Activity
- Full Agonists
- Partial Agonists
Mechanism of Action
Here we take an example of Salbutamol
Salbutamol:
- Stimulates beta-2 adrenergic receptors
- Activates adenylate cyclase
- Increases cyclic AMP (cAMP)
- Causes relaxation of bronchial smooth muscle
- Leads to bronchodilation
Clinical Effect
- Rapid airway opening
- Relief from breathlessness
- Quick action in asthma attacks
These drugs are especially useful as reliever medications in asthma.
Example Salbutamol
A complete guide on β₂-Agonists bronchodilators mechanism and classification can be read here
Anticholinergics
A complete guide on Anticholinergics mechanism and classification can be read here
Example: Ipratropium
Normally, acetylcholine (a neurotransmitter) binds to M3 muscarinic receptors in the airways and causes bronchoconstriction.
Mechanism of Action
Ipratropium:
- Blocks M3 muscarinic receptors
- Prevents the action of acetylcholine
- Reduces bronchoconstriction
- Causes bronchodilation
Clinical Effect
- Prevents airway narrowing
- Reduces mucus secretion
- Improves airflow
Anticholinergics are very effective in COPD management.
Methylxanthines
Example: Theophylline
Methylxanthines work by increasing the level of cAMP inside airway smooth muscle cells.
Mechanism of Action
Theophylline:
- Inhibits phosphodiesterase (PDE)
- Prevents breakdown of cAMP
- Increases cAMP levels
- Causes smooth muscle relaxation
- Leads to bronchodilation
Additional Effects
- Mild anti-inflammatory action
- Improves diaphragm contraction
However, methylxanthines have a narrow therapeutic index, meaning toxicity can occur at higher doses.
Summary:
| Class | Main Action | Example | Main Use |
|---|---|---|---|
| Beta-2 Agonists | Stimulate beta-2 receptors | Salbutamol | Acute asthma relief |
| Anticholinergics | Block M3 receptors | Ipratropium | COPD |
| Methylxanthines | Increase cAMP (PDE inhibition) | Theophylline | Chronic respiratory disease |
FAQs – Bronchodilators Mechanism and Classification
1. What are bronchodilators?
Bronchodilators are drugs that relax the smooth muscles of the bronchi and widen the airways, making breathing easier.
2. Where are bronchi located?
Bronchi are air-conducting tubes inside the lungs that carry air from the trachea into both lungs.
3. How do bronchi become narrow?
Bronchi become narrow due to:
- Smooth muscle contraction
- Inflammation (swelling of airway walls)
- Excess mucus production
These changes reduce airflow and cause breathing difficulty.
4. What causes airway narrowing in asthma and COPD?
Airway narrowing is caused by:
- Allergic reactions (asthma)
- Smoking and pollution (COPD)
- Infection
- Chronic inflammation
5. What are the main types of bronchodilators?
Bronchodilators are classified into three main types:
- Beta-2 agonists
- Anticholinergics
- Methylxanthines
6. How do beta-2 agonists work?
Beta-2 agonists stimulate beta-2 receptors in bronchial smooth muscle, increase cAMP levels, and cause muscle relaxation leading to bronchodilation.
Example: Salbutamol.
7. How do anticholinergics work?
Anticholinergics block M3 muscarinic receptors and prevent bronchoconstriction, helping the airways remain open.
Example: Ipratropium.
8. How do methylxanthines cause bronchodilation?
Methylxanthines inhibit phosphodiesterase (PDE), increase cAMP levels, and relax airway smooth muscle.
Example: Theophylline.
9. Which bronchodilator is used for quick relief in asthma?
Short-acting beta-2 agonists like Salbutamol are used for rapid relief during asthma attacks.
10. What are the common side effects of bronchodilators?
Common side effects include:
- Tremors (beta-2 agonists)
- Dry mouth (anticholinergics)
- Nausea and arrhythmia (methylxanthines)


2 thoughts on “Bronchodilators Mechanism and Classification: Types, Pharmacology and their Clinical Uses”